


The principle of distraction osteogenesis is a well-known principle since many decades.
It is important, in my opinion, to distinguish between the principles and the methods of limb lengthening. Limb lengthening uitilizes the principle of distraction osteogenesis (DO). The (DO) principle is applied with different methods. Although the principle of distraction osteogenesis remained unchanged, the methods and devices of fixing the bone and controlling the distraction have evolved through the years. Ilizarov initially used an external circular frame to fix the bone and to control its distraction and external ring fixators have been the only option of fixation until the late 1990’s when intramedullary nails start to be introduced. The methods of applying the principle of (DO) are better discribed in the article Methods of Bone Fixation in Limb Lengthening
DO was first discovered in the 1950’s by Professor Gavril Ilizarov in the former Soviet Union. Because of the political isolation in the years of the Cold war, it wasn’t until the 1980’s that the principle was introduced to the West.
The principle dictates that when a long bone is carefully broken (osteotomized) by the surgeon and the two parts of the bone are then slowly pushed away from each other (distracted), with a rate of around 1mm per day, normal bone is gradually formed in the developing gap. The bone eventually heals in an elongated position.
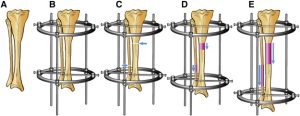
A: Before, B: Fixation of bone, C: Osteotomy, D and E: Distraction
The soft tissues (i.e. skin, muscles, nerves, vessels) also respond to the continuous tension and and they gradually elongate and adapt. Because the lengthening occurs in all tissues and not just the bone, the term “histogenesis” is used by some surgeons instead of “osteogenesis” (“histo-” means “tissue” in Greek).
Distraction osteogenesis is basically intervening and harnessing a natural healing response of the human body ( i.e. the ability of a broken bone to heal) and directing it towards a desired outcome with the help of human-made means.
Many parameters affect the outcome of the distraction osteogenesis and have been being studied continuously through the years. Some of those parameters are:
- The rate of daily lengthening.
- The surgical technique of the osteotomy.
- The location of the osteotomy.
- The condition of the soft tissue around the bone.
- The effect of growth factors, hormones and medications.
- The type and mechanical properties of the fixation.
- The patient’s compliance.
These parameters are discussed below, in the relevant phases of DO:
Phases of Distraction Osteogenesis
Surgery
What Is The Best Location To Divide The Bone?
Although the choice of the osteotomy site ultimately relies on the localization of the deformity, one should also take into consideration the pathological and histological characteristics of metaphyseal and diaphyseal bone. Metaphyseal bone is more vascularized, has a larger cross-section providing better stability and possesses thinner cortices, which are easier to separate.
However, the location of this bone leaves little room for fixation. Surgeons should perform metaphyseal osteotomies when addressing juxta-articular deformities or when doing straight lengthening. On the contrary, diaphyseal bone allows more room for fixation but has a smaller cross-section and is less bioactive. Indications for diaphyseal osteotomies should be limited to addressing only diaphyseal deformities.7,8,9
Methods of bone separation that disrupt the periosteum, such as significantly displaced corticotomies or osteotomies, can result in decreased osteogenesis.15
References
7. Aronson J, Harp JH. Mechanical forces as predictors of healing during tibial lengthening by distraction osteogenesis. Clin Orthop Relat Res. 1994; 301:73-79.
8. Aronson J, Good B, Stewart C et al. Preliminary studies of mineralization during distraction osteogenesis. Clin Orthop Relat Res. 1990; 250:43-49.
9. Hasler C, Krieg A. Current concepts of leg lengthening. J Child Orthop. 2012; 6(2):89-104.
15. Herzenberg JE, Waanders NA. Calculating rate and duration of distraction for deformity correction with the Ilizarov technique. Orthop Clin North Am. 1991; 22(4):601-611.
Latency
The latency phase starts immediately following the osteotomy and lasts between five and seven days. This stage resembles the acute stage of fracture repair with the formation of hematoma, inflammatory response and subsequent differentiation of stem cells into chondrocytes and osteoblasts.8 Pro-inflammatory cytokines interleukin-1 and 6 (IL-1 and IL-6), which are involved in bone repair, upregulate in this phase in order to promote periosteal callus formation. The expression of tumor necrosis factor (TNF) and recruitment of mesenchymal stem cells in the latency period supplements the organization and recruitment of inflammatory and mesenchymal cells as the bone segments prepare for distraction. An abbreviated form of this latency phase will risk the lack of bone formation and a prolonged phase can result in premature consolidation.11
References
8. Aronson J, Good B, Stewart C et al. Preliminary studies of mineralization during distraction osteogenesis. Clin Orthop Relat Res. 1990; 250:43-49.
11. Velazquez RJ, Bell DF, Armstrong PF et al. Complications of use of the Ilizarov technique in the correction of limb deformities in children. J Bone Joint Surg Am. 1993; 75(8):1148-1156.
Distraction
Following the latency period is the distraction phase. Distraction of the two bone segments starts at a specific rate and rhythm, typically at 1.0 mm a day, divided into four increments. Although 1 mm/day is classically cited, in practice the rate of distraction varies depending on multiple factors (patient age, health, medications, location of osteotomy, the type of osteotomy performed, etc.). In the foot and ankle, the distraction rate can range from 0.5 mm/day to 1 mm/day. The distraction phase consists of resorption of the periosteal callus and the formation of a fibrous interzone, comprised of types 1, 2, 4 and 10 collagen, oriented parallel to the distraction force.12
Probably the most distinguishing feature of the distraction phase involves the presence of angiogenesis and neoangiogenesis, regulated by the expression of vascular endothelial growth factor (VEGF) and angiopoietin signaling pathways.11 New blood vessels grow in loops along and between the collagen fibers, and allow osteoblasts to be recruited to the area. This fibrous interzone thus acts as a scaffold for the new bone formation, which forms by intramembranous ossification whereby bone forms directly from osteoblasts.
This is in distinct contrast to fracture healing whereby bone forms primarily by endochondral ossification using a cartilage template. In various animal models, researchers have shown that the expression of numerous growth factors related to osteogenesis and chondrogenesis upregulate, thus driving the process of intramembranous ossification.13,14 These include bone morphogenetic proteins (BMP-2, BMP-4), and growth factors including transforming growth factor beta (TGF-beta), fibroblast growth factor (FGF), insulin growth factor (IGF) and platelet derived growth factor (PDGF).
Key Insights On Distraction Rate And Rhythm
The effect of the rate and rhythm for distraction osteogenesis has a significant effect on the expression of factors involved in the distraction osteogenesis process. Schiller and coworkers examined the alteration of expression of various growth factors in rapid distraction in comparison to routine distraction.13 Furthermore, several experimental studies have shown improved bone regeneration using continuous versus intermittent distraction osteogenesis with the former demonstrating upregulation of several growth-stimulating genes.16 Schiller and coworkers found there was decreased cellular staining of fibroblast growth factor, vascular endothelial growth factor, and platelet-derived growth factor in the rapid distraction group starting on the first day of lengthening.13
There are numeric parameters to quantify the quality and speed of bone formation. Authors most widely use the healing index parameter and define it as the time needed for consolidation per centimeter of the distracted osteotomy site.15 Consolidation time is defined as the time between the end of distraction and total consolidation or removal of hardware. The consolidation time is about twice as long as the distraction time in children but may be three to four times longer in adults.15 Accordingly, it usually amounts to one month/cm in children and two to three months/cm in adults.17
References
11.Velazquez RJ, Bell DF, Armstrong PF et al. Complications of use of the Ilizarov technique in the correction of limb deformities in children. J Bone Joint Surg Am. 1993; 75(8):1148-1156.
12. Vauhkonen M, Peltonen J, Karaharju E, et al. Collagen synthesis and mineralization in the early phase of distraction bone healing. Bone Miner. 1990; 10(3):171-81.
13. Schiller JR, Moore DC, Ehrlich MG. Increased lengthening rate decreases expression of fibroblast growth factor 2, platelet-derived growth factor, vascular endothelial growth factor, and CD31 in a rat model of distraction osteogenesis. J Pediatr Orthop. 2007; 27(8):961-8.
14. Hamdy RC, Rendon JS, Tabrizian M. Distraction osteogenesis and its challenges in bone regeneration. Bone Regeneration, InTech. 2012; 185-212.
15. Herzenberg JE, Waanders NA. Calculating rate and duration of distraction for deformity correction with the Ilizarov technique. Orthop Clin North Am. 1991; 22(4):601-611.
16. Peacock ZS, Tricomi BJ, Murphy BA, et al. Automated continuous distraction osteogenesis may allow faster distraction rates: a preliminary study. J Oral Maxillofac Surg. 2013; 71(6):1073-84.
17. Ilizarov GA. The tension-stress effect on the genesis and growth of tissues. Part 1. The influence of stability of fixation and soft tissuepreservation. Clin Orthop Rel Res. 1989; 238:249-281.
Consolidation
Once you have achieved the desired amount of lengthening, the distraction phase stops and the consolidation phase begins. During the consolidation phase, osteoid (unmineralized bone matrix) that osteoblasts laid down becomes progressively mineralized. An increase in the expression of TNF-alpha regulates consolidation and the downregulation of BMP expression.11 TNF-alpha controls remodeling of the regenerated bone by coordinating the coupled action of osteoclasts and osteoblasts. This is the longest phase in distraction osteogenesis, allowing approximately one month for each centimeter lengthened.4
References
4. Goldstein RY, Jordan CJ, McLaurin TM, et al. The evolution of the Ilizarov technique; Part 2: The principles of distraction osteosynthesis. Bull Hosp Jt Dis. 2013; 71(1):96-103.
11. Velazquez RJ, Bell DF, Armstrong PF et al. Complications of use of the Ilizarov technique in the correction of limb deformities in children. J Bone Joint Surg Am. 1993; 75(8):1148-1156.
References
- Ilizarov GA. The tension-stress effect on the genesis and growth of tissues: part II. The influence of the rate and frequency of distraction. Clin Orthop Relat Res (1989) 239:263–85.
- Ilizarov GA. Clinical application of the tension-stress effect for limb lengthening. Clin Orthop Relat Res (1990) 250:8–26.
Go back to Limb Lengthening- introduction